Bell's Palsy: Coping With Unnerving Facial Paralysis
Date
July 1, 2025
Credits

Date
July 1, 2025
Credits
Medical providers featured in this article
In Brief
{{cta-block}}
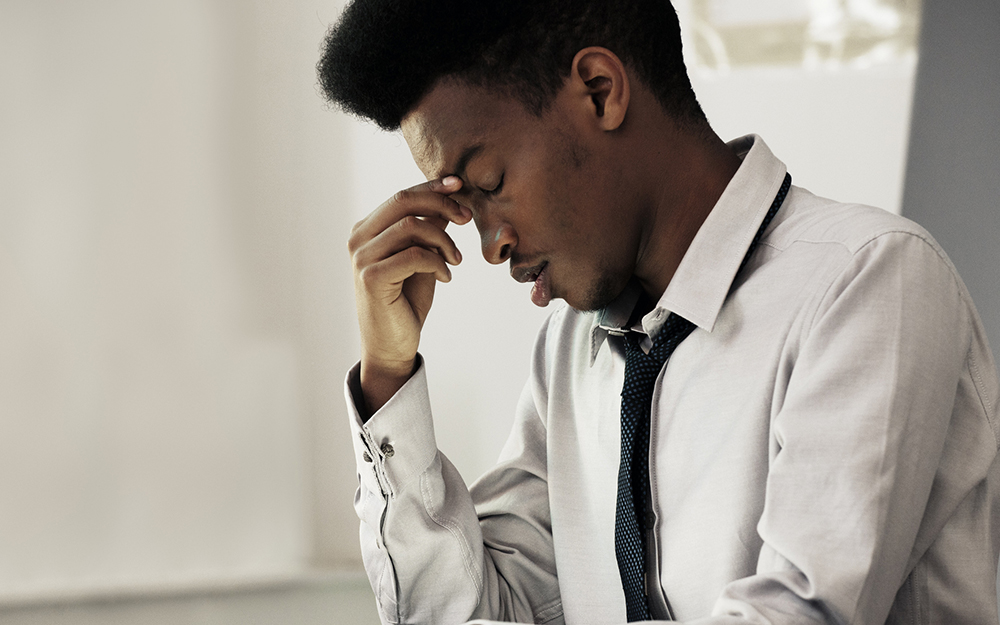
When we look in the mirror, we expect to see a familiar face. But with Bell’s palsy, you can wake up to an unfamiliar, alarming reflection: eyebrows, eyelids and mouth drooping on one side, as if your face got stuck overnight.
Around 40,000 Americans develop this abrupt facial paralysis every year and often don’t know what’s happening. The neurological disorder occurs when the nerve that powers facial muscles, allowing you to smile, squint and move your face, turns off or is damaged. As a result, the affected muscles weaken, and the condition typically reaches a peak in severity within 24 to 72 hours.
“Don’t just wait out facial paralysis to see if it goes away,” urges Cedars-Sinai neurologist Paula Barreras, MD.
She emphasized that you should take these sudden symptoms seriously. The vast majority of people with Bell’s palsy, though, make a full recovery.
{{providers}}
Facing Fear
The exact reasons for the interrupted nerve communication are unclear, but experts point to inflammation of the facial nerve. Pregnancy and preeclampsia triple your likelihood of Bell’s palsy, while the National Institute of Neurological Disorders and Stroke notes risk also rises with:
- High blood pressure
- Diabetes
- Obesity
- Upper respiratory infections, such as the flu
The phenomenon—which overwhelmingly strikes between the ages of 15 and 45—can temporarily freeze one side of your face. Losing control of how you express yourself can be disturbing.
“Although it looks dramatic and severe, when it’s truly Bell’s palsy, it’s a benign syndrome that in most cases will get better,” Barreras said. “Understanding that can help ease anxiety and uncertainty.”
She recommends watching your facial changes closely for subtle warning bells: Facial nerve palsies cause paralysis in both your upper and lower face, restricting closing of the eyes. But weakness that is limited to just the bottom of your face is a sign of stroke. If you can freely move your forehead—or notice any accompanying neurological symptoms, such as double vision or numb or weak limbs—seek emergency care.
“Don’t just wait out facial paralysis to see if it goes away.”
Look After Your Eyes
Facial nerve fibers send many messages from the brainstem to your eyes, ears, tongue and mouth. When that network stops communicating, Bell’s palsy interferes with sensation and protective tear and salivary glands.
Food can taste different, or you might lose taste altogether. Some hear noise very loudly on one side of their ear (hyperacusis). People often drool, ache and develop dry mouth and eyes.
Barreras stresses that eye care is vital: Hydrate daily with eye drops and longer-lasting, specialized ointments at night. She also suggests taping your eyes or using a patch, if closing them is difficult.
“If you don't take care of your eye, the dryness and constant exposure can lead to problems in your cornea and ulcers,” she said.
When It’s Not Just Bell’s Palsy
Bell’s palsy is the most common, but not the only, cause of facial paralysis. Neurological evaluation is essential for recognizing complex syndromes.
“Bell’s palsy is used as a final diagnosis, and it shouldn’t be: There are many causes of facial weakness,” Barreras said.
To get a clearer picture of nerve damage, neurologists use a physical exam, medical history, blood tests and neurodiagnostic tools such as a spinal tap or MRI with contrast when there are red flags.
Infections and disordered immune responses both fuel inflammation and are common triggers of facial weakness. For example, herpes and varicella zoster virus (the virus that causes chickenpox and shingles) can infect a facial nerve. Called Ramsay Hunt syndrome, these viral complications tend to be more painful and severe, often causing fever, nausea, vertigo and a rash of mouth and ear blisters or ulcers. Lyme disease can similarly inflame the facial nerve.
“Everyone’s allowed to have one episode of Bell’s palsy or facial weakness that doesn’t have an identifiable cause,” Barreras explained.
But if it happens twice—even if it’s been years—or progresses, your doctor needs to rule out other serious conditions. Autoimmune diseases, cancers and trauma that press on or damage facial nerves, or trigger swelling in the meninges (the brain’s protective layer), can mimic Bell’s palsy.
“Whenever somebody tells me they have had Bell’s palsy, I always pause and screen for signs and symptoms of a chronic inflammatory condition called sarcoidosis,” cautioned Barreras.
Immune Defense
Facial paralysis from Bell’s palsy is typically treated with a one-to-two-week course of anti-inflammatory oral steroids such as prednisone, alongside antiviral medications for severe cases.
Muscle control should start to return within a month to six months. With the right quick-healing steps, almost 95% of people regain function.
Experts recommend starting treatment within three days, particularly if your case is infectious or severe. See an ophthalmologist regularly to ensure you don’t have permanent vision problems. Some people develop weepy “crocodile tears” in one eye—an unusual response to salivating and chewing—as they recover. Another complication is synkinesis, when nerve function returns muddled and connected to the wrong feature. Your eye might close when you smile, or your whole face might spasm.
Botox injections freeze unwanted, reflexive contractions, making expressions more symmetrical. Together with talk therapy, treatment can improve your longest-lasting relationship—with yourself.