November 2022
Clinical History
A female patient in her 70s presented to her gynecologist complaining of intermittent lower abdominal pain, bulk symptoms, cramping, and vaginal spotting for 6 months. Her medical history is significant for breast cancer diagnosed over 10 years ago and class II obesity. The patient underwent a pelvic ultrasound which revealed an 8 mm endometrial stripe and a 7 cm x 5 cm left uterine mass [figure 1] deemed a uterine fibroid. Endometrial biopsy showed carcinosarcoma and the patient subsequently underwent hysterectomy and bilateral salpingo-oophorectomy. The tumor measured 11.5 x 10.0 x 3.1 cm and was semi-firm, tan-white, friable, and exophytic on gross examination. F myometrial invasion into the serosa and involvement of bilateral ovaries and fallopian tubes was identified. [figure 2]
Microscopic examination confirmed carcinosarcoma [figure 3] and revealed heterologous elements, including osteosarcoma and chondrosarcoma [figure 4 and 5]. Metastatic carcinomatous component was identified in the right ovary (1.0 cm) [figure 6], left ovary (0.2 cm), as well as right para-ovarian tissue with tumor cells residing in lymphovascular spaces. The tumor was staged at pathological stage pT3a and a FIGO stage IIIA: local and/or regional spread of the tumor, invading serosa of the corpus uteri and/or adnexa. Finally, the patient was started on adjuvant chemotherapy with carboplatin and paclitaxel.
Discussion
Definition
Uterine carcinosarcoma (UCS), formally known as malignant mixed Müllerian tumor, is a neoplasm characterized by both carcinomatous and sarcomatous elements. The carcinomatous component is most frequently of serous or high-grade endometrioid morphology, but may be of clear cell, or undifferentiated types and often coexist within the same tumor [1]. The sarcomatous component may be classified as either homologous, meaning mesenchymal differentiation elements intrinsic to the uterine stroma (e.g., endometrial stromal sarcoma, leiomyosarcoma, undifferentiated sarcoma) or heterologous, extrinsic to uterine stroma. Heterologous elements include rhabdomyosarcoma, chondrosarcoma, osteosarcoma, liposarcoma, or fibrosarcoma [1]. Due to the morphologic heterogeneity of UCS, accurate histologic diagnosis is limited by pre-operative endometrial sampling and a definitive histological diagnosis is often made after hysterectomy [2].
Epidemiology
UCS accounts for ~5% of uterine malignancies in the United States with the average age of diagnosis at 65. Predisposing factors for UCS do not significantly differ from endometrial carcinoma, and include obesity, nulliparity, use of exogenous estrogen, tamoxifen therapy, postmenopausal age, and history of pelvic radiation [3].
Presentation
Patients' initial symptoms are often postmenopausal vaginal bleeding, abdominal pain, or vaginal discharge. Approximately 50% of patients are found to have an enlarged uterus on physical exam and/or a polypoid lesion protruding from the endocervical canal [4]. Grossly, carcinosarcomas are bulky and often resemble carcinoma, manifesting as a polypoid lesion filling the endometrial cavity and frequently deeply invading the myometrium [3].
Pathophysiology
Recent genetic studies have identified that carcinosarcoma arises from a single malignant epithelial clone that subsequently undergoes mesenchymal transdifferentiation (EMT). Mutations in KRAS and TP53 as well as patterns of X-chromosome inactivation and loss of heterozygosity shared between both the carcinomatous and sarcomatous components supports a theory of monoclonal origin [5]. This may account for the similarities in epidemiology, risk factors, and clinical behavior to endometrial carcinoma as opposed to uterine sarcomas.
Prognosis
USC is an aggressive neoplasm with a median overall survival of less than 2 years and a 5-year survival rate between 5% to 35% at all stages [6]. Stage, sarcomatous dominance (>50% of tumor), and tumor size (≥5 cm), are the most important prognostic factors for patients with USC. Staging is by the same FIGO/TNM classification system as for endometrial carcinoma [7,8]. Lymphovascular space invasion and deep myometrial invasion to the outer half layer of the uterine wall occurs in up to 50% of cases [6]. The presence of heterologous elements, particularly rhabdomyoblasts, is associated with a more aggressive clinical course, therefore immunostaining for skeletal muscle markers (desmin, myoglobin, myogenin, Myo-D1) is recommended for establishing differentiation when suspected. It is the carcinomatous component that has the highest propensity to invade and is found at metastatic sites [3].
Treatment
The mainstay of treatment is a total abdominal hysterectomy, bilateral salpingo-oophorectomy, with or without pelvic and para-aortic lymph nodes dissection in addition to surgical staging (peritoneal washing cytology or peritoneal biopsies). Current National Comprehensive Cancer Network practice guidelines list the combination of carboplatin/paclitaxel as a category 1 recommendation for UCS [6].
Updates
Overexpression of HER2 has been reported in up to 10% to 25 % of UCS making anti-HER2 therapies a potential target [8,9,10] Epithelial cell adhesion molecule (EpCAM) has been found to be overexpressed in about 80 % of UCS making it a potential target for Solitomab, a bispecific antibody construct against EpCAM and CD3 [8,11]. Approximately 20% of UCS are MSI-H, 10% of UCS are POLE-ultramutated, and about 60% have PD-1 and PD-L1 (Programmed death ligand 1) expression, all indicators of immune checkpoint inhibitors as possible therapeutic options. Finally, inhibiting pathways of EMT may lead to the regression of sarcomatous elements and improve treatment efficacy. It is speculated that TGF-β may play a role in EMT, therefore TGF-β inhibitors such as galunisertib, when used in combination with carboplatin/paclitaxel, may significantly improve treatment [8].
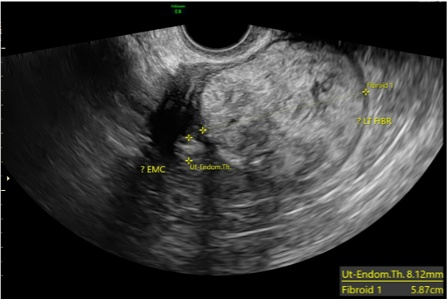
Figure 1. Pelvic ultrasound demonstrates a 7.82 x 5.87 cm mass with an 8.12 mm thickened endometrial stipe.

Figure 2. Gross photograph of semi-firm, polypoid, friable tumor filling up the endometrial cavity with full thickness invasion to the serosa, and involvement of bilateral fallopian tubes and ovaries.
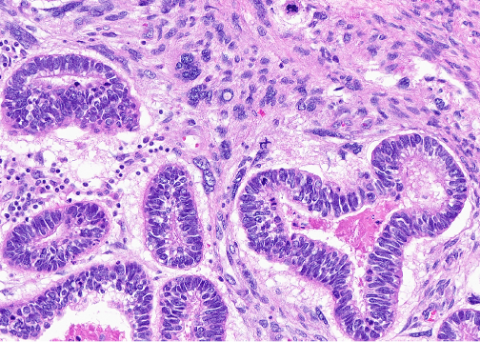
Figure 3. Medium power view of high-grade malignant stroma surrounding malignant high-grade glandular epithelium arranged in a biphasic pattern.
The stromal component above reflects a homologous undifferentiated sarcoma composed of polymorphous round to spindled cells with large vesicular nuclei, coarse chromatin, scant cytoplasm, and readily identifiable mitotic figures. The epithelial component above demonstrates serous carcinoma, however, can be composed of endometrioid, clear cell, or squamous carcinoma.
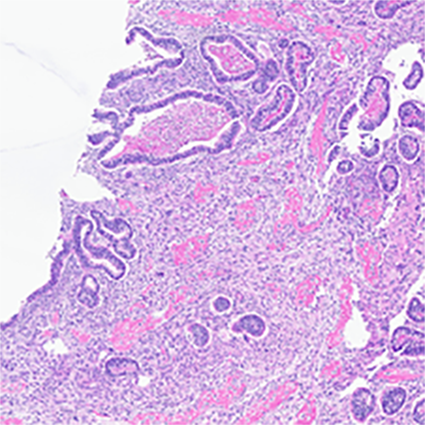
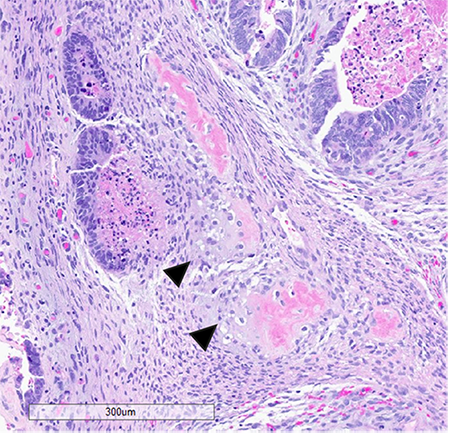
Figure 4 (left) and figure 5 (right): The sarcomatous component in this case showed heterologous elements in the form of osteosarcoma, large, atypical cells resembling osteoblasts with densely eosinophilic cytoplasm forming osteoid (fig. 3) and chondrosarcoma, atypical, neoplastic chondrocytes, and islands of mature appearing, well differentiated hyaline cartilage (fig. 4 arrow heads)
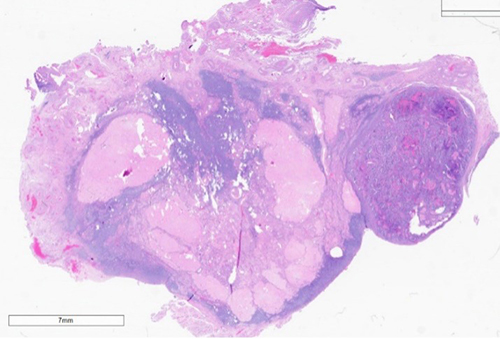
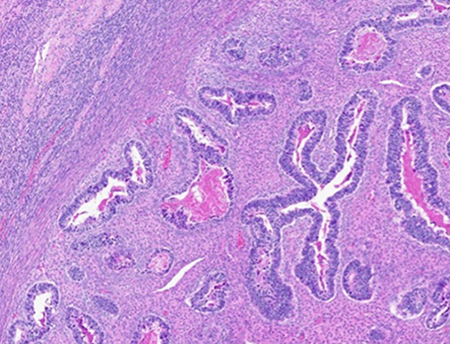
Figure 5: Low power (left) and high power (right) view of metastatic carcinomatous component to the right ovary. It is the epithelial component which has the greatest propensity to invade and metastasize.
References
- Matias-Guiu, Xavier & Parra-Herran, Carlos. (2020). Endometrial Glandular Neoplasia. 10.1016/B978-0-323-35909-2.00010-2.
- Bansal N, Herzog TJ, Seshan VE, et al. Uterine carcinosarcomas and grade 3 endometrioid cancers: evidence for distinct tumor behavior. Obstetrics and Gynecology. 2008;112(1):64–70
- Christopher D.M. Fletcher MD, FRCPath Diagnostic Histopathology of Tumors Fifth Edition Tumors of the Female Genital Tract. Chapter 13, pages 702-912
- Leigh A. Cantrell, Stephanie V. Blank, Linda R. Duska, Uterine carcinosarcoma: A review of the literature, Gynecologic Oncology, Volume 137, Issue 3, 2015, Pages 581-588, ISSN 0090-8258, https://doi.org/10.1016/j.ygyno.2015.03.041.
- Pezzicoli G, Moscaritolo F, Silvestris E, Silvestris F, Cormio G, Porta C, D'Oronzo S. Uterine carcinosarcoma: An overview. Crit Rev Oncol Hematol. 2021 Jul; 163:103369. doi: 10.1016/j.critrevonc.2021.103369. Epub 2021 May 27. PMID: 34051304.
- R.L. van der Horst, O. van der Hel, L. Lutgens, M. van der Aa, B. Slangen, R. Kruitwagen and R.I. Lalisang. The role of multimodal adjuvant therapy for FIGO I-II carcinosarcoma of the uterus: a systematic review. Critical Reviews in Oncology and Hematology, 2022-07-01, Volume 175, Article 103701, Copyright © 2022
- Nemani D, Mitra N, Guo M, Lin L. Assessing the effects of lymphadenectomy and radiation therapy in patients with uterine carcinosarcoma: a SEER analysis. Gynecol Oncol. 2008 Oct;111(1):82-8. doi: 10.1016/j.ygyno.2008.05.016. PMID: 18674808.
- Matsuzaki S, Klar M, Matsuzaki S, Roman LD, Sood AK, Matsuo K. Uterine carcinosarcoma: Contemporary clinical summary, molecular updates, and future research opportunity. Gynecol Oncol. 2021 Feb;160(2):586-601. doi: 10.1016/j.ygyno.2020.10.043. Epub 2020 Nov 9. PMID: 33183764.
- Menderes G, Clark M, Santin AD. Novel targeted therapies in uterine serous carcinoma, an aggressive variant of endometrial cancer. Discov Med. 2016 Apr;21(116):293-303. PMID: 27232515.
- Nicoletti R, Lopez S, Bellone S, Cocco E, Schwab CL, Black JD, Centritto F, Zhu L, Bonazzoli E, Buza N, Hui P, Mezzanzanica D, Canevari S, Schwartz PE, Rutherford TJ, Santin AD. T-DM1, a novel antibody-drug conjugate, is highly effective against uterine and ovarian carcinosarcomas overexpressing HER2. Clin Exp Metastasis. 2015 Jan;32(1):29-38. doi: 10.1007/s10585-014-9688-8. Epub 2014 Nov 15. PMID: 25398397; PMCID: PMC4310789.
- Ferrari F, Bellone S, Black J, Schwab CL, Lopez S, Cocco E, Bonazzoli E, Predolini F, Menderes G, Litkouhi B, Ratner E, Silasi DA, Azodi M, Schwartz PE, Santin AD. Solitomab, an EpCAM/CD3 bispecific antibody construct (BiTE®), is highly active against primary uterine and ovarian carcinosarcoma cell lines in vitro. J Exp Clin Cancer Res. 2015 Oct 17; 34:123. doi: 10.1186/s13046-015-0241-7. PMID: 26474755; PMCID: PMC4609066.