July 2022
Clinical History
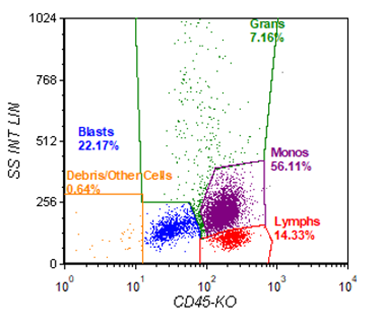
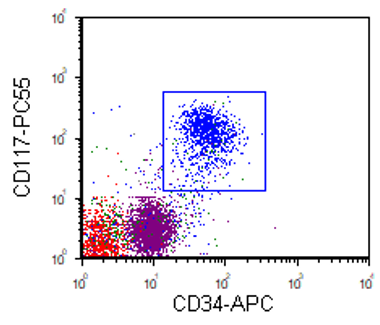
A patient in their 60’s with recently diagnosed reactive arthritis who presented to an OSH with intermittent fever and chills. At OSH, was found to have a WBC of 56.11 and was started on hydroxyurea. Bone marrow biopsy at OSH showed left-shifted maturation with a 33% blast differential consistent with acute myeloid leukemia with monocytic differentiation. Patient was transferred to Cedars for increased level of care.
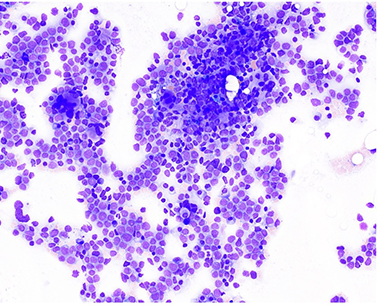
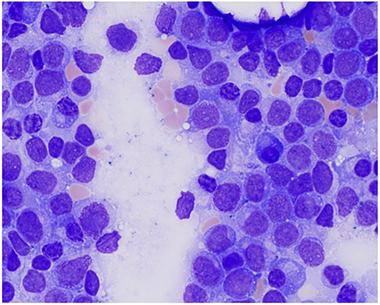
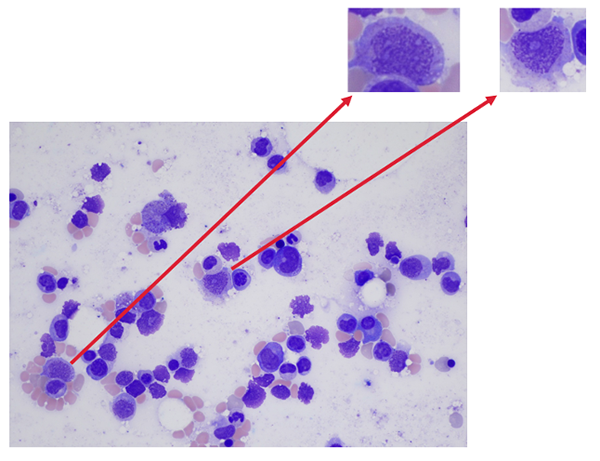
Bone Marrow Biopsy:
Increased blasts and increase promonocytes consistent with AMML. Monocytosis also noted.
Initial Molecular Findings:
TET2 (Y1598Ifs*12) – 45.4%
SRSF2 (P95H) – 41.6%
RUNX1 (D93GFs*30) – 40.7%
RUNX1 (M371Rfs8225) – 40.6%
ASXL1 (G646Wfs*12) – 32.3%
Clinical Course:
Started on chemotherapy for AML. Post-induction (day 30) biopsy showed no evidence of residual disease by MRD flow cytometry or morphology. Another bone marrow biopsy was performed following consolidation therapy in preparation for an allogenic SCT.
Post-Consolidation MRD Flow Cytometry: No evidence of residual disease
Post Consolidation Morphology: 8-10% blasts/promonocyte equivalents – concern for residual disease
Post-Consolidation Molecular Findings:
TET2 (Y1598Ifs*12) – 87.4%
SRSF2 (P95H) – 44.7%
ASXL1 (G646Wfs*12) – 36.6%
RUNX1 (H404Pfs*196) – 16.5%
The patient underwent allo-HSCT.
60 days post-transplant, patient had no evidence of residual disease by molecular, morphology, or MRD flow cytometry.
Discussion
The importance of measurable residual disease (MRD) testing in AML has been well documented over the past decade, with MRD+ patients at the end of induction or consolidation having significantly worse outcomes compared to MRD- patients1. AML MRD testing is primarily limited to flow cytometry or NGS due to the heterogenous nature of AML. Currently, MRD flow cytometry is more sensitive for AML MRD testing compared to NGS. However, with the decreasing costs of sequencing, increasing sequencing depth to increase sensitivity is becoming more feasible.
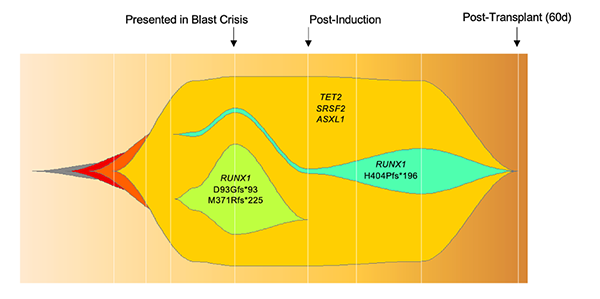
The patient series presented here highlights the necessity for incorporation of morphology, molecular, and flow cytometry for detection of residual disease, especially in AML with monocytic differentiation. Based on the presenting genetics in this case, it is likely that this patient’s AMML arose from an underlying CMML (TET2, SRSF2 and ASXL1) mutations. The blast crisis most likely emerged following the evolution of a clone which gained two RUNX1 mutations. Following induction, the blast population was depleted, but the underlying CMML genetics remained. These underlying genetics possibly allowed the emergence of an underlying clone with a new driver mutation (RUNX1 H404Pfs*196). While this clone was able to be detected by NGS, AML with monocytic maturation is very difficult to detect by MRD flow cytometry, further exemplifying the need for an integrative process in patient management.
References
- Short NJ, Zhou S, Fu C, et al. Association of Measurable Residual Disease With Survival Outcomes in Patients With Acute Myeloid Leukemia: A Systematic Review and Meta-analysis. JAMA Oncol. 2020;6(12):1890–1899. doi:10.1001/jamaoncol.2020.4600