December 2023 Case
Clinical History
Patient in his 70’s with an extensive past complex medical history who in the last few years presented with intractable mid abdominal pain. After workups, imaging showed a mass in the hepatic lobe. Ultrasound suggested hemangioma. After biopsy was done neuroendocrine tumor was diagnosed. After being admitted for management of acute pancreatitis, and he underwent EGD/EUS with core biopsy. EUS revealed a 4 x 3 cm hypoechoic mass in the uncinate process of the pancreas involving the splenic vein. Core biopsy showed well-differentiated neuroendocrine tumor, intermediate grade, Ki-67 ~ 17%. NGS was done and found tumor mutation burden of 10 mut/Mb, with alterations including MSH6. Multiple chemo regimens were given, and he was doing well. Around early 2021 Pembrolizumab, Temozolomide along with capecitabine was started. Mid 2023, a second round of Temozolomide was given. Late 2023 the patient presented with abdominal pain and liver mass which core biopsy showed high grade neuroendocrine neoplasm, Ki-67 ~ 76%, consistent with chemoresistance. NGS showed a dramatic jump of TMB from 10.5 to 134, and same MSH6 as the previous study. Mutation signature showed an enriched C>T substitutions (Fig 1). What explains TMB surge / C>T enriched signature and treatment resistance?
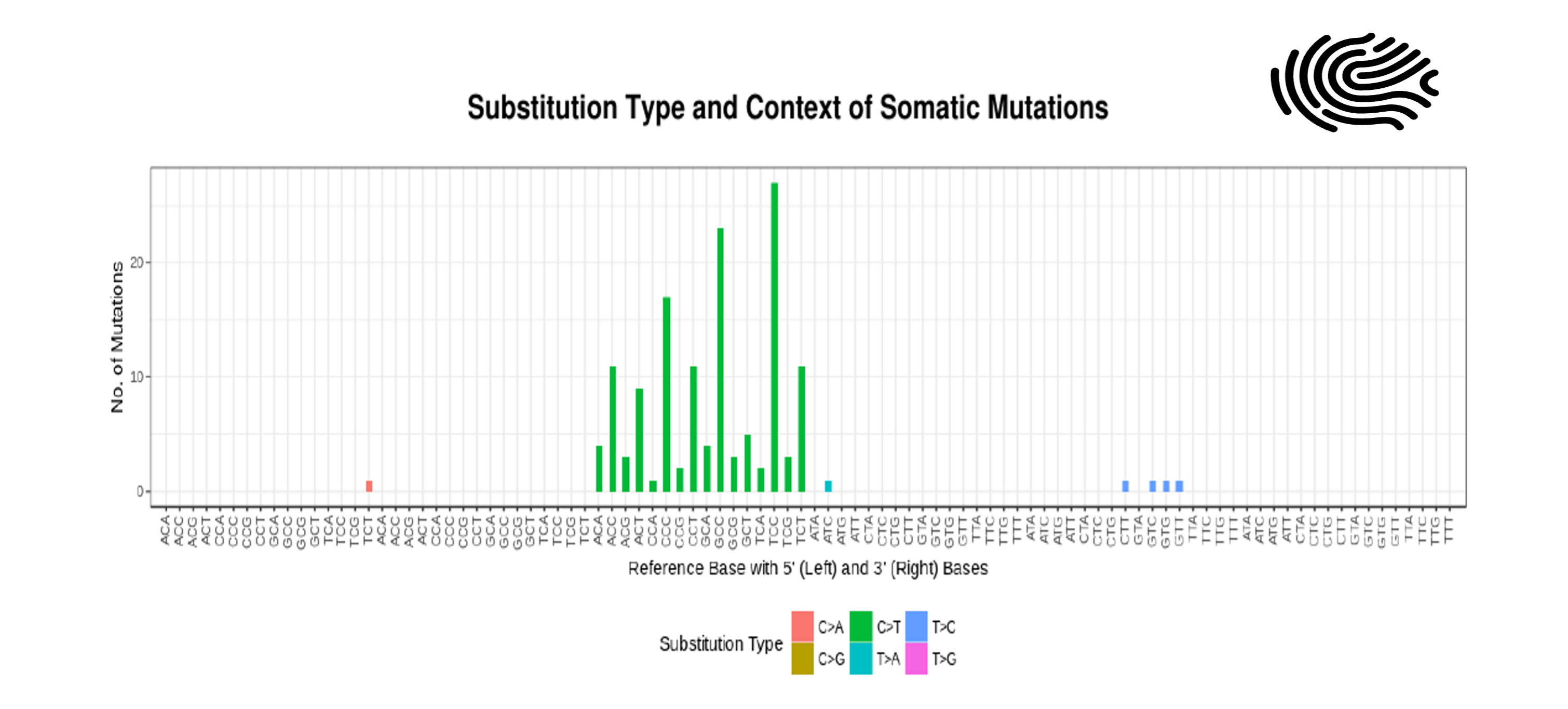
Fig1: Mutational pattern resembling that of alkylating agents. This signature is enriched for C>T substitutions on guanine bases due to transcription-coupled nucleotide excision repair. A strong transcriptional strand-bias is present in this signature. Link to compare with cosmic alkylating signature: https://cancer.sanger.ac.uk/signatures/sbs/sbs11/.
Diagnosis
TMZ induced hypermutation/signature and resistance.
Definition: TMZ-induced hypermutation is defined by a dramatic increase in the mutation rate and a TMZ-associated mutational signature in posttreatment recurrences. Secondary defective MMR (in this case MSH6 mutation) leads to the resistance.
Discussion
Tumor Mutational Burden (TMB) can be defined as the total number of somatic coding non-synonymous mutations. Whole exome sequencing is the gold standard method. It correlates with high levels of neoantigens and tumor infiltrating lymphocytes. Has been shown to predict patients' response to immunotherapy. Usually clinically reported as High, Intermediate or Low. These categories are test dependent.
Temozolomide (TMZ) monotherapy and the combination of TMZ and capecitabine have indeed shown promising clinical activity in the treatment of both low- and high-grade neuroendocrine neoplasms (NENs). It's noteworthy that high-grade NENs have traditionally shown limited responsiveness to immune checkpoint inhibitor (ICI) monotherapy, possibly due to lower tumor mutational burden (TMB). Temozolomide (TMZ) monotherapy and the combination of TMZ and capecitabine have shown clinical activity in both low- and high-grade neuroendocrine neoplasms (NENs). These treatments are considered among the available options for managing neuroendocrine tumors. Temozolomide is an alkylating agent that has demonstrated efficacy in the treatment of neuroendocrine tumors by inhibiting DNA synthesis, and when used in combination with capecitabine, which is an oral chemotherapy drug, it can enhance therapeutic outcomes.
Temozolomide (TMZ) is known to be mutagenic, and its mutagenic effects are particularly observed at CpC and CpT dinucleotides. TMZ is an alkylating agent, and its therapeutic mechanism involves introducing methyl groups into the DNA, which can lead to DNA damage. This methylation can result in base pair mismatches, specifically at CpC and CpT sites, leading to mutagenesis. This explains the increase in TMB, and this is the basis of preparing the cells for immunotherapy.
In cancers, acquired mutations that inactivate the DNA mismatch repair (MMR) pathway, including genes like MSH6, have been identified as mechanisms of resistance to TMZ. The MMR pathway is responsible for correcting errors that occur during DNA replication, and when it is compromised, cells may become resistant to the effects of TMZ, as they are less able to repair the DNA damage induced by the drug and harbor more and more of mutations(Fig 2).
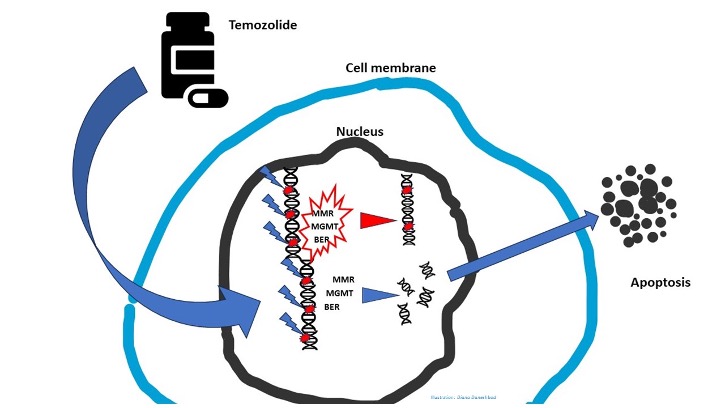
Fig2: Temozolomide's Mechanism of Action-Temozolomide enters the nucleus. Then, it moves methyl groups on to guanine, causing DNA breaks during replication and leading to apoptosis. Resistance/ineffective drug is caused by defects in any of these intranuclear DNA repair mechanisms, including MGMT, MMR, and BER.
BER = base excision repair; MGMT = 06-methylguanine-DNA methyltransferase; MMR = mismatch repair, MTIC = 3-methyl- (triazen-1-yimidazole-4-carboxamide.
Mutation signature is based on the six substitution subtypes: C>A, C>G, C>T, T>A, T>C, and T>G, as well as the nucleotides immediately 5’ and 3’ to the mutation. A mutational signature is the outcome of a mutagenic process comprising some form of DNA damage, subsequently acted upon by DNA repair and/or replicative machinery. Our patient exhibits a mutational pattern resembling that of alkylating agents. This signature usually generates large numbers of somatic mutations (>10 mutations per MB), in line with post TMZ high TMB. This signature is enriched for C>T substitutions on guanine bases due to transcription-coupled nucleotide excision repair. A strong transcriptional strand-bias is present in this signature. Mutational signatures, which represent distinct patterns of genetic mutations, offer valuable insights into the underlying biological mechanisms involved in both carcinogenesis and normal somatic mutagenesis. Understanding the specific mutational landscape of a tumor can guide therapeutic strategies and aid in the development of preventive measures. Mutational signature profiling has proven successful in identifying candidates for immunotherapy, particularly in cancers with mismatch repair deficiency.
References
- Klempner SJ, Hendifar A, Waters KM, Nissen N, Vail E, Tuli R, Mita A. Exploiting Temozolomide-Induced Hypermutation With Pembrolizumab in a Refractory High-Grade Neuroendocrine Neoplasm: A Proof-of-Concept Case. JCO Precis Oncol. 2020 Nov; 4:614-619.
- Johnson BE, Mazor T, Hong C, et al: Mutational analysis reveals the origin and therapy-driven evolution of recurrent glioma. Science 343:189-193, 2014
- Yip S, Miao J, Cahill DP, et al: MSH6 mutations arise in glioblastomas during temozolomide therapy and mediate temozolomide resistance. Clin Cancer Res 15:4622-4629, 2009
- Koh G, Degasperi A, Zou X, Momen S, Nik-Zainal S. Mutational signatures: emerging concepts, caveats and clinical applications. Nat Rev Cancer. 2021 Oct;21(10):619-637. doi: 10.1038/s41568-021-00377-7. Epub 2021 Jul 27. PMID: 34316057.
- COSMIC | SBS11 - Mutational Signatures (sanger.ac.uk)