April 2023 Case
Background
Lung cancer is the second most common malignancy diagnosed amongst men and women in the United States1. In the hopes of catching lung lesions at an early stage, the USPSTF recommended annual CT screening for current and former smokers aged 50 to 802. These screenings, in addition to the widespread adoption of CT scans, has led to an increase in the discovery of pulmonary nodules requiring biopsies. Historically, a transthoracic approach was used to biopsy peripheral lesions, however, in recent years, the FDA approved the use of a robotic navigated bronchoscopic approach for aspirations and biopsies. This new approach has the capability of reaching small peripheral lung nodules with a lower risk of complications and allows the option of proceeding directly into more definitive surgery under the same anesthetic event3,4.
Clinical History
A female in her 60s with a 30-year smoking history, COPD and emphysema was found to have a 1.9 x 1.6 cm right lower lobe solitary lung nodule on CT imaging of the chest. The patient presented for a robotic navigated bronchoscopic aspiration and biopsy. Three passes were sent for intraoperative cytology adequacy and assessment. On low power, the smears showed sheets and clusters of small, bland appearing cells (Figure 1A). On higher power, loosely cohesive clusters and dispersed single cells with nuclear enlargement, hyperchromasia, and moderate cytoplasm were appreciated. Some cells showed a plasmacytoid appearance (Figure 1B-D). The differential diagnosis included typical and atypical carcinoid, granular cell tumor, plasmacytoma, and neuroendocrine carcinoma, amongst others. Given the lack of necrosis and no evident increase in mitosis, a low-grade neoplasm, favor carcinoid, defer to permanent was rendered. There was no concurrent surgical frozen.
For the final cytology diagnosis, a total of 6 direct smears, one SurePath, and one cell block preparation were examined. The aspirate showed a monomorphic population of cells present in sheets with round to oval, centrally placed nuclei and abundant cytoplasm. On the cell block, the cells demonstrated anastomosing cords of cells (Figure 2A). Immunohistochemical stains, HepPar, polyclonal CEA, and TTF-1 were ordered on the cell block. The cells were positive for HepPar and CEA, while negative for TTF-1 (Figure 2B-D). The final diagnosis was benign hepatocytes consistent with liver sampling. The concurrent surgical biopsy showed benign bronchial wall with mild chronic inflammation.
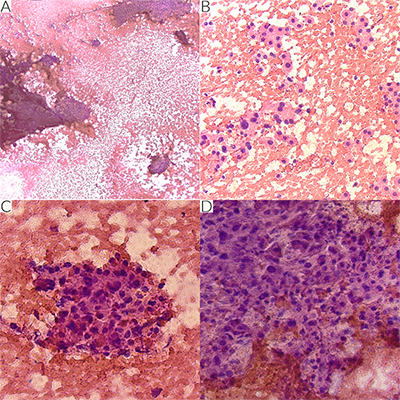
Figure 1 Intraoperative smears stained with H&E. Sheets and clusters of fairly small, bland appearing cells x 4x (A). Cells appear loosely cohesive and as dispersed individual cells with enlarged hyperchromatic nuclei showing moderate nuclear pleomorphism. Some cells have a plasmacytoid appearance x 20x (B-D).
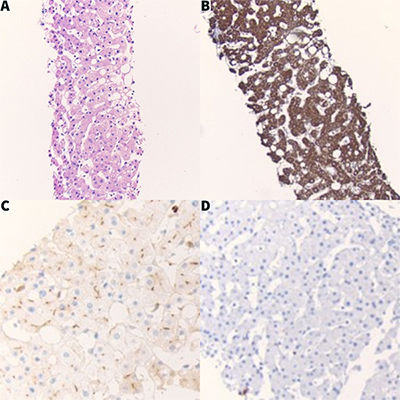
Figure 2 Cell block preparation. The cell block showed anastomosing cords of bland polygonal cells (A), and immunohistochemical stains revealed cytoplasmic staining with HepPar (B), canalicular staining with polyclonal CEA, and lack of staining with TTF-1 (D). This staining pattern supports the diagnosis of benign liver hepatocytes.
Discussion
While striking, this case was one of only two false positive diagnoses of malignancy during intraoperative diagnosis. Over the course of approximately two years, 466 total lung lesions were sampled using the robotic navigated bronchoscopic approach, with 24% of the targets in the right lower lobe. Nearly 91% of the total lesions were sent for intraoperative cytology assessment with a 62% concordance rate with final cytology diagnosis, rendering a 66% and 99% sensitivity and specificity, respectively. This case demonstrates that even with advancing technology, we may not always receive representative samples from the targeted lesion and to keep the regional anatomy in mind when approaching cases.
References
- Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin 2023;73(1):17-48. DOI: 10.3322/caac.21763.
- Pham D, Bhandari S, Pinkston C, Oechsli M, Kloecker G. Lung Cancer Screening Registry Reveals Low-dose CT Screening Remains Heavily Underutilized. Clin Lung Cancer 2020;21(3):e206-e211. DOI: 10.1016/j.cllc.2019.09.002.
- Gould MK, Tang T, Liu IL, et al. Recent Trends in the Identification of Incidental Pulmonary Nodules. Am J Respir Crit Care Med 2015;192(10):1208-14. DOI: 10.1164/rccm.201505-0990OC.
- Agrawal A, Hogarth DK, Murgu S. Robotic bronchoscopy for pulmonary lesions: a review of existing technologies and clinical data. J Thorac Dis 2020;12(6):3279-3286. DOI: 10.21037/jtd.2020.03.35.