April 2021 Case
Authors
Vimal Krishnan, MD (Fellow), Souzan Sanati (Faculty)
Cytopathology
Clinical History
A male patient in his 40s presented initially for right upper quadrant pain. On ultrasound, an abdominal hematoma was found and drained. Following several episodes of recurrent hematoma, additional imaging studies were performed. A CT scan revealed multiple lesions in the liver as well as retroperitoneal lymphadenopathies. A fine needle aspiration and core biopsy of one of the liver lesions was performed.
Microscopic findings
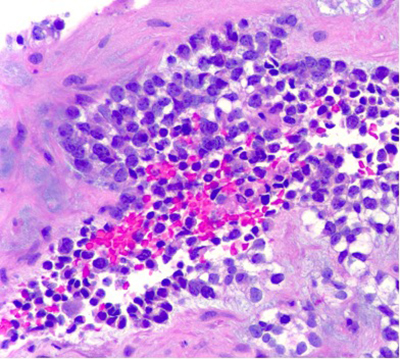
The aspirate was hypercellular and composed of small round cells, distributed in clusters of loosely cohesive clusters and as isolated cells. Moderate pleomorphism, hyperchromasia and variably prominent nucleoli were noted. On cell block preparation, the cytoplasm of these cells had a cleared appearance. Geographic necrosis was noted, with viable cells present in perivascular areas. Focally, there was an extracellular myxoid matrix.
Ancillary studies
The differential diagnosis for this small round cell tumor was wide and includes carcinoma, sarcoma, melanoma, lymphoma and germ cell tumors. Immunohistochemical studies were performed and were negative for hepatocytic markers (Hepar, arginase-1), keratins (AE1/AE3, OSCAR, CAM5.2, CK8/18), EMA, neuroendocrine markers (chromogranin, synaptophysin, TTF1) melanoma markers (S0X10, HMB-45, Melan-A, S100), lymphoid marker (CD45), germ cell markers (SALL4, OCT3/4) and muscular markers (myogenin, desmin). INI1 was preserved. CD99 showed focal weak positive staining.
In light of the morphologic findings and the focal staining for CD99, a diagnosis of Ewing sarcoma was considered. Fluorescent in-situ hybridization (FISH) studies using a EWSR1 break-apart probe was negative (no rearrangement). A sarcoma fusion analysis panel by next-generation sequencing was performed and revealed a CIC-DUX4 fusion.
Diagnosis
Undifferentiated round cell sarcoma with CIC-DUX4 translocation.
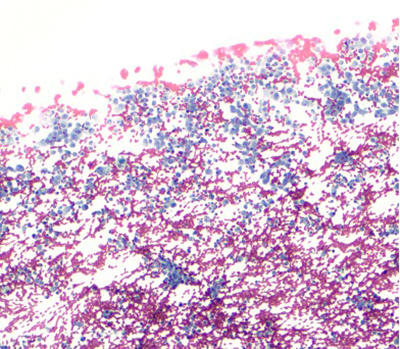
Papanicolaou stain (100X)
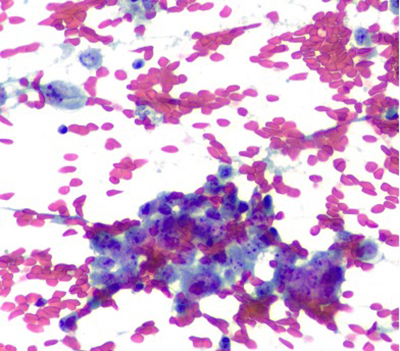
Papanicolaou stain (400X)
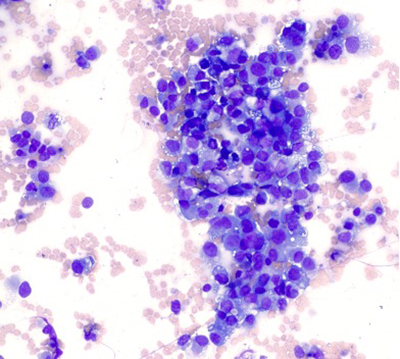
Giemsa stain (400X)
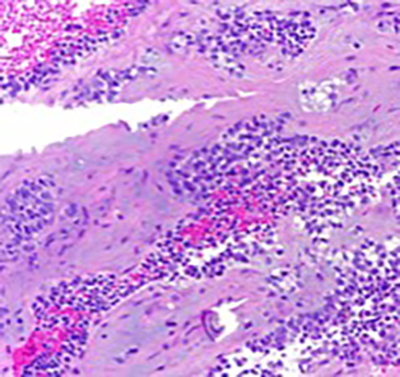
Cell block preparation (200X)
Cell block preparation (400X)
Discussion
The Ewing family of sarcomas includes Ewing sarcoma, defined by a EWSR1 rearrangement, as well as other recently described EWSR1-negative sarcomas. Two-thirds of these tumors have the CIC-DUX4 translocation. Other reported fusions involved BCOR (BCOR-CCNB3, BCOR-MAML3 and ZC3H7B-BCOR).
CIC is a transcriptional repressor located on chromosome 19. Loss of function mutations have been described in oligodendrogliomas and other tumors. DUX4 is a double homeobox transcription factor, normally expressed in germ cells but epigenetically silenced in differentiated somatic cells. Two translocations have been described for CIC-DUX4 fusion sarcomas: t(4;19)(q35;q13) and t(10;19)(q26;q13). A study on cell lines showed that this fusion results in transcriptional upregulation of the PEA3 family of transcription factors, which are overexpressed in several malignancies.
The differential diagnosis is vast and includes many tumors that can present as small round cells, including conventional Ewing sarcoma. Recent studies have shown that CIC-DUX4 fusion sarcomas are clinically and morphologically different from Ewing sarcoma. CIC-DUX4 fusion sarcoma tends to arise deep in the soft tissue and in older patients (median: 40 years old), whereas Ewing sarcoma (median: 15 years old) arises in the bone in younger patients. Morphologically, the tumor cells exhibit mild pleomorphism, vesicular chromatin with variably prominent nucleoli, moderate amount of light eosinophilic cytoplasm and stroma with myxoid change. This is in contrast to Ewing sarcoma, which is usually monotonous with inconspicuous nucleoli. The immunohistochemical profile is also different. CD99 shows strong membranous staining in Ewing sarcoma, but is weak and variable in CIC-DUX4 fusion sarcoma. WT1 is usually negative in Ewing but is positive in most cases of CIC-DUX4 sarcoma. Recently, DUX4 immunohistochemistry has been shown to be positive, reflecting the fusion driving tumorigenesis. Molecular testing is ultimately required to identify one of the diagnostic translocations.
The importance in recognizing this new entity lies in its prognostic significance. A large study by Antonescu and colleagues examined this issue in a study of 115 cases. CIC-DUX4 fusion sarcoma had a 5-year overall survival of 43%. This is notably worse than conventional Ewing sarcoma, which had a 5-year overall survival of 76%. Pathologic response to neoadjuvant chemotherapy was poor in 70% of these cases. This tumor also showed a higher metastatic rate, mainly to the lung.
Overall, this case underscores the morphologic, immunohistochemical and molecular findings of CIC-DUX4 fusion sarcoma, an aggressive tumor in the family of EWSR1-negative sarcomas.
References
- Antonescu CR, Owosho AA, Zhang L, Chen S, Deniz K, Huryn JM, Kao YC, Huang SC, Singer S, Tap W, Schaefer IM, Fletcher CD. Sarcomas With CIC-rearrangements Are a Distinct Pathologic Entity With Aggressive Outcome: A Clinicopathologic and Molecular Study of 115 Cases. Am J Surg Pathol. 2017 Jul;41(7):941-949. doi: 10.1097/PAS.0000000000000846. PMID: 28346326; PMCID: PMC5468475.
- Miettinen M, Felisiak-Golabek A, Luiña Contreras A, Glod J, Kaplan RN, Killian JK, Lasota J. New fusion sarcomas: histopathology and clinical significance of selected entities. Hum Pathol. 2019 Apr;86:57-65. doi: 10.1016/j.humpath.2018.12.006. Epub 2019 Jan 8. PMID: 30633925; PMCID: PMC7443750.
- Kawamura-Saito M, Yamazaki Y, Kaneko K, Kawaguchi N, Kanda H, Mukai H, Gotoh T, Motoi T, Fukayama M, Aburatani H, Takizawa T, Nakamura T. Fusion between CIC and DUX4 up-regulates PEA3 family genes in Ewing-like sarcomas with t(4;19)(q35;q13) translocation. Hum Mol Genet. 2006 Jul 1;15(13):2125-37. doi: 10.1093/hmg/ddl136. Epub 2006 May 22. PMID: 16717057.