September 2020 Case
Authors
Andrea Krajisnik, MD, MS (Resident), Eric Vail, MD (Faculty)
Molecular Pathology
Clinical History
Female in mid-forties with past medical history of asthma, ocular migraines, and mononucleosis who presented with respiratory symptoms. Subsequent evaluation revealed incidentally elevated hemoglobin of three weeks duration.

Molecular analysis for JAK2 V617F mutation was performed but no mutation was identified. Additional testing was ordered to assess for possible mutations in MPL or CALR, but these findings were also normal. To exclude the possibility of elevated hemoglobin in the setting of chronic myeloid leukemia (CML), RT-PCR analysis for BCR-ABL1 fusion was performed. These findings showed no abnormalities. Finally, Myeloid NGS was performed which identified a 6 base pair deletion in exon 12 of JAK2 (p.N542_E543del).
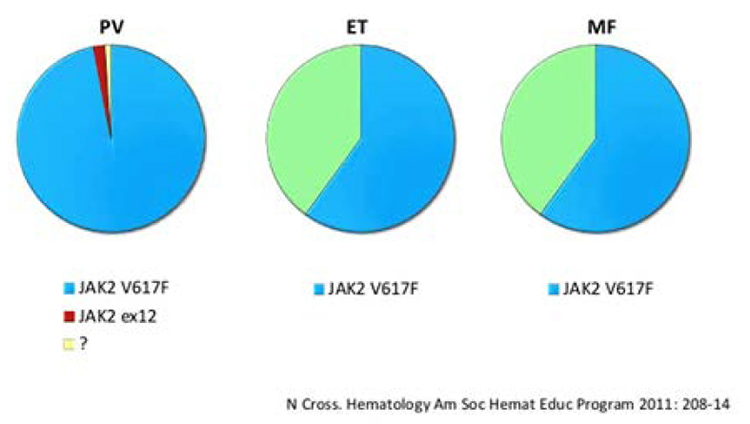
Incidence of JAK2 Mutations
Diagnosis
Polycythemia Vera (PV) secondary to JAK2 exon 12 alteration.
Discussion
Polycythemia Vera is a myeloproliferative disorder leading to the abnormal production of erythrocytes independent of the growth factor erythropoietin (EPO). The vast majority of patients with PV carry an acquired mutation of JAK2 V617F. PV is a slowly progressing disease and diagnosis is usually delayed to around age 60. Patients may be identified on the basis of lab abnormalities alone, or may present with headaches, blurry vision, fatigue, abnormal bleeding, thrombosis or a variety of other symptoms related to the bloods compromised ability to travel through vessels to various sites in the body.
The diagnosis of PV is most often confirmed on the basis of PCR-based sequencing of DNA from leukocytes to evaluate for the presence of mutations in codon 617 of JAK2. If testing is negative, additional studies can be performed in conjunction with the clinical presentation. This testing evaluates other possible causes for hematologic disturbances related to myeloproliferative disorders including BCR-ABL1 rearrangements and mutational analysis of CALR and MPL. JAK2 exon 12 alterations are also identified in approximately 5% of patients with PV.
JAK2 exon 12-mutated PV is important to recognize as these patients may present at an earlier age. Additionally, their mean hemoglobin and hematocrit levels tend to be more elevated that those patients with the more common JAK2 V617F mutation. Despite these differences, both JAK2 mutations have similar rates of thrombosis, disease progression, and death. The accurate diagnosis of this disorder relies on an understanding of possible etiologies and a thorough molecular investigation.