May 2020 Case
Clinical History
A male patient in his 50s with gout, dyslipidemia, reactive airway disease, and contact with a family member who tested positive for COVID-19, presents to the emergency department with productive cough, nausea, vomiting, diarrhea, fevers, chills, myalgias, and generalized weakness.
The patient has no history of diabetes, hypertension, or kidney disease. The only medicines he takes are Tramadol for generalized pain and allopurinol for gout. He denies NSAID use.
The patient has no known drug allergies. He has no family history of kidney disease. He admits to smoking tobacco and denies any illicit drug use.
On physical examination he appears acutely ill and the remainder of the physical exam is deferred. Following intravenous administration of 1 L of normal saline, vitals are notable for temperature of 38.8 C, heart rate of 92 beats per minute, respiratory rate of 20 breaths per minute, blood pressure of 123/73, and O2 saturation of 93% on 2-4 L O2 via nasal cannula.
Laboratory studies are notable for normal Hb, normal WBC and Plt counts, and normal PT, PTT, and INR. Blood gas and chemistry show metabolic acidosis and respiratory alkalosis. He has a serum creatinine of 11.3 mg/dL, and on urinalysis there are moderate blood, 3+ protein, and no leukocytes.
A chest x-ray shows bilateral patchy infiltrates, consistent with pneumonitis. Influenza A and B PCR assays are negative, and a COVID-19 PCR assay is ordered.
A renal biopsy is performed to assess for presumed rapidly progressive glomerulonephritis/pulmonary renal syndrome. Following renal biopsy, the COVID-19 PCR assay returns positive.
Renal Biopsy
In the specimen for light microscopy, three glomeruli show segmental to global collapsing features with epithelial cell hypertrophy, hyperplasia, mitoses, and cytoplasmic protein droplets (Figure 1A). Uninvolved glomeruli are mildly enlarged and with smooth, single-contoured capillary walls. A single capillary loop in a patent glomerulus is thrombosed (Figure 1B), without evidence of associated basement membrane disruption or necrosis. There is no mesangial expansion, hypercellularity, typical segmental sclerosis, necrosis, or crescentic injury. There is minimal parenchymal scarring. Tubular epithelial cells are attenuated and necrotic with regenerative/degenerative nuclear atypia (Figure 1C). There is frequent tubular luminal necrotic debris, and several tubular epithelial cells contain prominent coarse protein resorption droplets. No microcystically dilated tubules are identified. The interstitium displays patchy mild to moderate edema and multifocal mild inflammation composed of lymphocytes with few plasma cells. One arteriole is thrombosed. There is mild arterial and arteriolar sclerosis. No vascular inflammation is identified.
No glomerular immune complex staining is identified by immunofluorescence microscopy.
On electron microscopy, there is near complete effacement of podocyte foot processes, accompanied by podocyte microvillous transformation (Figure 1D). Endothelial cells show segmental loss of fenestrae and swelling. There is no subendothelial lucent material, mesangial interposition, or basement membrane duplication. Numerous tubuloreticular inclusions are readily identified in peritubular capillary and glomerular capillary endothelial cell cytoplasm (Figure 1E). There are no electron dense (immune complex) deposits. No definitive viral particles are identified.
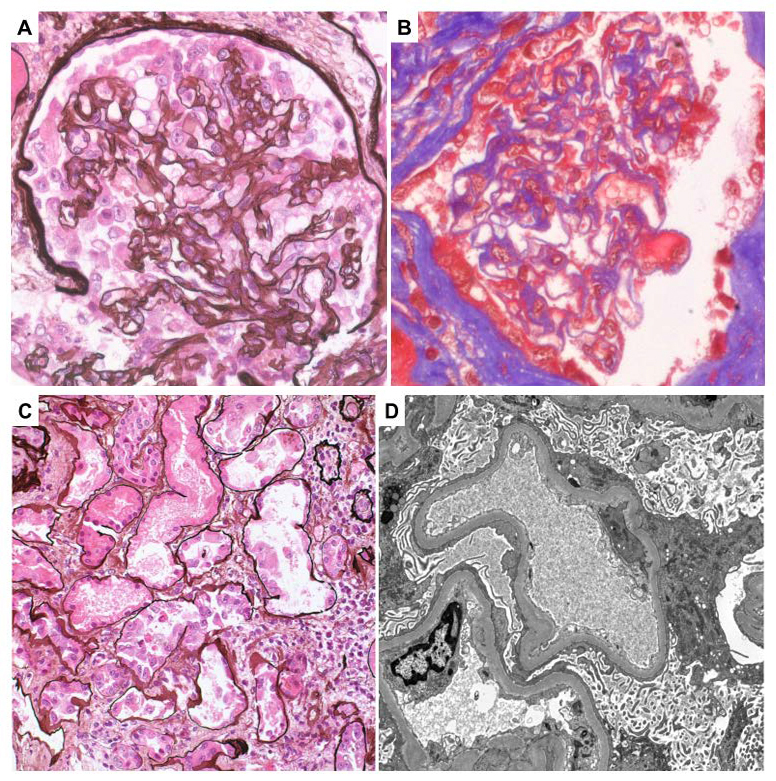
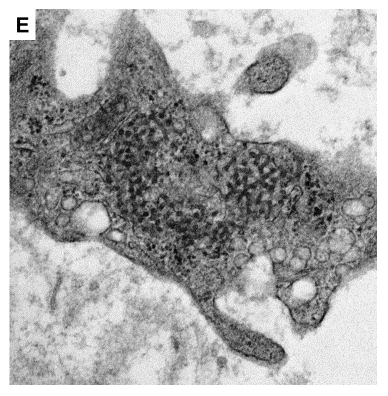
Figure 1. Renal biopsy findings. A) Silver stain of glomerulus with tuft collapse and epithelial cell hyperplasia and hypertrophy. B) Trichrome stain of glomerulus with a thrombosed capillary loop. C) Silver stain of tubules with epithelial shedding and denudation of basement membranes. D) Transmission electron micrograph of complete podocyte foot process effacement with microvillous transformation. E) Transmission electron micrograph of tubuloreticular inclusion in peritubular capillary endothelial cell cytoplasm.
Diagnosis
Collapsing glomerulopathy, acute tubular necrosis, and thrombotic microangiopathy.
Discussion
Here we present a case of a COVID-19 positive male patient in his 50s with respiratory and gastrointestinal symptoms, found to have new onset renal failure with hematuria and heavy proteinuria. Renal biopsy showed collapsing glomerulopathy, acute tubular necrosis, and thrombotic microangiopathy. No viral particles were identified in the biopsy tissue by electron microscopy. Below we give a brief primer on the clinicopathologic features of collapsing glomerulopathy and thrombotic microangiopathy, followed by a summary of emerging features in reports of kidney pathology in COVID-19 patients.
Collapsing glomerulopathy is histologically defined by the presence of at least one glomerulus with segmental or global tuft collapse (loss of patency of glomerular capillary lumina) with accompanying epithelial cell hypertrophy and hyperplasia, forming a “pseudocrescent.” These glomerular findings are often seen in association with acute tubular injury, coarse tubular protein reabsorption droplets, tubular microcysts, and interstitial inflammation. Complete podocyte foot process effacement is often seen on electron microscopy. In most case series, collapsing glomerulopathy is more common is young to middle-aged males of African ancestry, who typically present with nephrotic syndrome. Clinical course is aggressive with low percentage of disease remission with immunosuppressive therapy, and prognosis is poor with median renal survival of 13 to 15 months. A number of nuclear and mitochondrial genotypes have been linked to collapsing glomerulopathy, including APOL1 genotypes increased in frequency in individuals of African descent. Known secondary triggers of collapsing glomerulopathy include infections (particularly viral infections such as HIV and Parvovirus B19), autoimmune disease (lupus), inflammatory conditions (hemophagocytic lymphohistiocytosis), hematopoietic malignancies, medications (pamidronate and interferon therapy), and conditions causing acute glomerular ischemia.
Acute thrombotic microangiopathy is histologically defined by fibrin thrombi in glomerular capillaries, arterioles, and/or arteries. Thrombotic microangiopathy etiologies are histologically indistinguishable, and include malignant hypertension, antiphospholipid antibody syndrome, thrombotic thrombocytopenic purpura, infection-associated hemolytic uremic syndrome, inherited or acquired deficiencies in regulators of the alternative complement pathway, scleroderma renal crisis, drug (including interferon therapy) toxicity, radiation toxicity, and neoplasia.
While the effects of severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2) infection on the respiratory, immune, and coagulation systems are more well recognized, SARS-CoV-2 infection has also been associated with renal abnormalities. In large studies of hospitalized patients with COVID-19 in Wuhan, China, 44 to 59% had proteinuria, 27 to 44% had hematuria, and 3 to 7% developed acute renal failure [1–4].
A post mortem case series of 26 Chinese patients with fatal COVID-19 [5], identified acute tubular injury in all cases and thrombi in glomerular and peritubular capillaries in three (12%) cases. There are also three reports from the United States and Switzerland of collapsing glomerulopathy found on biopsy of COVID-19 patients with acute renal failure and proteinuria following or concomitant with respiratory symptoms [6–8]. In all three such case reports, patients were of African descent, and in two of the cases, genetic testing showed APOL1 genotypes associated with collapsing glomerulopathy [6,8]. Our case bears many similarities in patient demographics and clinical presentation to these case reports, although the APOL1 genotype of our patient is unknown. Unique to our case is that it manifests both the thrombotic microangiopathy described in the Chinese case series and the collapsing glomerulopathy described in the US and Switzerland case reports. Given that interferon stimulation is a predisposing factor to both thrombotic microangiopathy and collapsing glomerulopathy, it is appealing to speculate that the systemic interferon response triggered by SARS-CoV-2 is responsible for renal pathology in COVID-19 patients. Additional factors potentiating the development of collapsing glomerulopathy include cytokine storm due to SARS-CoV-2 infection and APOL1 risk alleles increased in frequency in individuals of African descent.
The mechanisms of kidney injury in SARS-CoV-2 infection have yet to be defined. Studies of the tissue distribution of the functional receptor for SARS-CoV2, angiotensin-converting enzyme 2 (ACE2), indicate receptor expression in both renal proximal tubules and podocytes, suggesting that direct renal infection could play a role in renal injury. Indeed, by electron microscopy, a number of groups have identified particles morphologically consistent with SARS-CoV-2 in both renal biopsies from living COVID-19 patients and post mortem specimens from patients with fatal COVID-19 infection. Groups have also demonstrated detection of the SARS-CoV-2 nucleoprotein in renal tissue by immunohistochemistry. Efforts to identify SARS-CoV-2 RNA in the kidney by in situ hybridization or nucleic acid amplification-based approaches, however, have been unsuccessful, calling into question the specificity of morphologic and immunohistochemical identification. Thus whether kidney injury in COVID-19 patients is by direct infection and/or secondary to cytokine storm remains an active area of research.
References
- Chen N, Zhou M, Dong X, et al (2020) Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. doi: 10.1016/S0140-6736(20)30211-7
- Huang C, Wang Y, Li X, et al (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. doi: 10.1016/S0140-6736(20)30183-5
- Wang D, Hu B, Hu C, et al (2020) Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA - J Am Med Assoc. doi: 10.1001/jama.2020.1585
- Cheng Y, Luo R, Wang K, et al (2020) Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int. doi: 10.1016/j.kint.2020.03.005
- Su H, Yang M, Wan C, et al (2020) Renal histopathological analysis of 26 postmortem findings of patients with COVID-19 in China. Kidney Int. doi: 10.1016/j.kint.2020.04.003
- Larsen CP, Bourne TD, Wilson JD, et al (2020) Collapsing Glomerulopathy in a Patient With Coronavirus Disease 2019 (COVID-19). Kidney Int Reports. doi: 10.1016/j.ekir.2020.04.002
- Kissling S, Rotman S, Gerber C, et al (2020) Collapsing glomerulopathy in a COVID-19 patient. Kidney Int. doi: 10.1016/j.kint.2020.04.006
- Peleg Y, Kudose S, D’Agati V, Siddall E, Ahmad S, Kisselev S, Gharavi A and Canetta P (2020) Acute Kidney Injury Due to Collapsing Glomerulopathy Following COVID-19 Infection. Kidney Int. Reports