December 2020 Case
Authors
Jayjay Z. Blanco, MD (Fellow); Danielle Ann Hutchings, MD (Faculty)
Gastrointestinal Pathology
Clinical History
This is a case of a female in her mid-thirties who presented to her primary care physician with complaints of "crampy" abdominal pain and diarrhea of unknown duration. No significant past medical or family history is noted. She was referred to a gastroenterologist for further evaluation and subsequently underwent an upper gastrointestinal endoscopy/esophago-gastro-duodenoscopy and colonoscopy which showed unremarkable findings of both the upper and lower gastrointestinal tract. Representative biopsies from the esophagus, stomach, duodenum, terminal ileum and colon were performed for histologic evaluation.
Histology/Immunohistochemistry
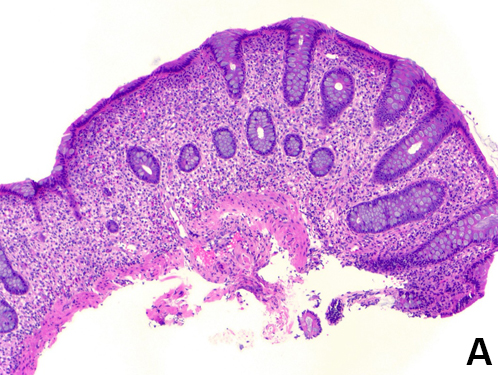
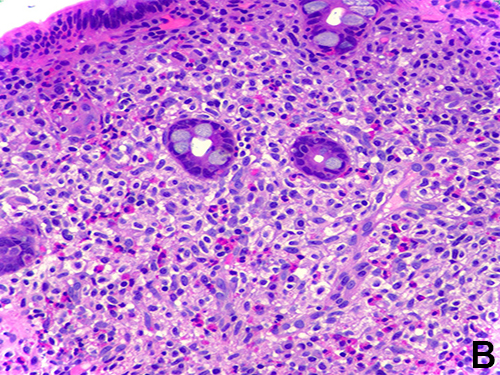
Figure 1. (A) Hematoxylin and eosin stain 20x. On lower magnification, there is increased lamina propria cellularity with a slight pale appearance. (B) Hematoxylin and eosin stain 40x. On higher magnification, the lamina propria infiltrate is composed of oval to spindled cells with clear cytoplasm accompanied by prominent eosinophils.
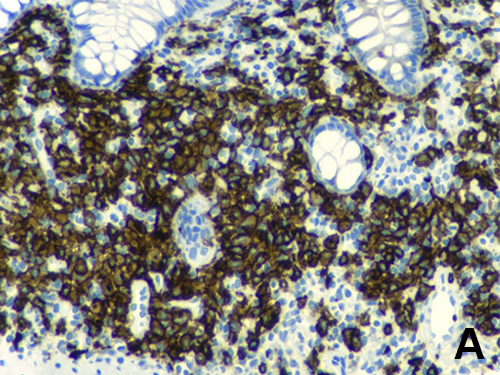
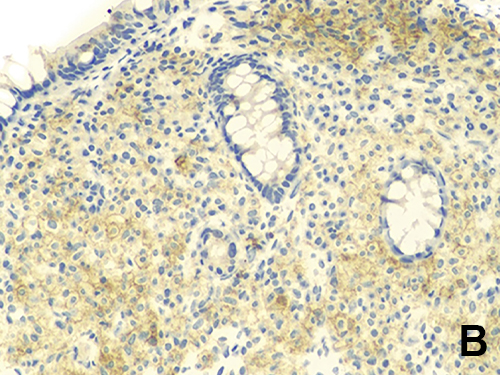
Figure 2. Immunohistochemical (IHC) stains. The cellular lamina propria infiltrate is highlighted by membranous staining of (A) CD117 IHC 40x and (B) CD25 IHC 40x; confirming that these are neoplastic mast cells. The mast cells may cluster around crypts as is seen here or show band-like infiltrate beneath the surface epithelium.
Diagnosis
Systemic mastocytosis involving colon
Discussion
Mastocytosis is described as a rare group of disorders in which proliferation of clonally mutated neoplastic mast cells accumulate in tissues. This can be limited to the skin (cutaneous mastocytosis, CM) also regarded to as urticaria pigmentosa or may involve multiple extracutaneous organs systems (systemic mastocytosis, SM), most commonly involving the bone marrow. In SM, the GI tract is involved in majority of patients (60-80%) with the colon (95%) being the most commonly affected area. Clinically, there is a wide range of symptoms including abdominal discomfort or pain, diarrhea, constipation, urgency or incontinence. Skin involvement may be absent at presentation in nearly half of all patients.
SM is generally diagnosed in the second decade of life and has a slight female predominance (0.67:1 male to female ratio). Based on the WHO, SM may manifest in distinct forms including indolent SM, SM with associated clonal hematologic nonmast cell lineage disease (SM-AHNMD) and aggressive SM and mast cell leukemia. The diagnosis requires either the presence of 1 major and 1 minor OR 3 minor criteria as follows: a) major criteria - multifocal dense mast cell infiltrates in tissue sections (≥ 15 cells) and b) minor criteria - > 25% spindle, immature, or atypical mast cells; detection of KIT D816V mutation, expression of CD25 &/or CD2 on mast cells and/or serum total tryptase persistently > 20 ng/mL (in absence of clonal myeloid disorder).
Most SM patients with GI tract involvement have indolent SM. In these cases, the symptoms are usually mild to moderate and can be managed symptomatically using histamine receptor H2 blockers. SM with predominant GI tract involvement does occur, but isolated involvement of the GI tract is uncommon, and infiltration of the bone marrow, even to a minimal degree, is found in almost all patients and a bone marrow biopsy is recommended as the optimal means of pursuing the diagnosis of SM.
Endoscopically, the colonic findings are non-specific but may include mucosal erythema, nodularity, ulceration, or stricture depending on site of disease involvement. Histologically, colonic biopsies show variable findings that can range from subtle to marked expansion of the lamina propria by increased numbers of oval, spindled mast cells with clear cytoplasm, commonly associated conspicuous eosinophilic infiltrate, and vague crypt architectural distortion. It is important to note, however, that increased mast cell numbers alone are not specific to mastocytosis and may be found in colonic biopsies from patients with inflammatory bowel disease, infections (parasitic or bacterial) or irritable bowel syndrome. Formation of compact micronodular or dense band-like infiltrates of mast cells is pathognomonic for mastocytosis and is not seen in mast cell hyperplasia. Currently, there is conflicting studies on evaluating mast cells in colonic biopsies and their corresponding diagnostic and prognostic implications.
Immunohistochemically, mast cells are positive for tryptase and C-kit (CD117) and show aberrant co-expression of CD25, which according to studies are diagnostic. This aberrant immunophenotype of mast cells is also commonly found in other tissues as well.
Prognosis depends on the type of SM and is accordingly very unfavorable in patients with advanced SM, whereas those with indolent SM usually have an almost normal life expectancy.
In conclusion, we present a unique case of systemic mastocytosis with an initial presentation involving the colon. The diagnosis of GI involvement by SM should be considered in GI biopsies of patients with prolonged, unexplained symptoms of pain and diarrhea, particularly in the setting of unremarkable or subtle endoscopic findings. Morphologic assessment with a high index of suspicion is key to this diagnosis. In suspected cases, ancillary studies including immunohistochemical stains, serum tryptase levels, and molecular assay for the KIT D816V mutation should be explored. While studies are still very limited and conflicting, more research needs to be done to enable better diagnostic criteria to aid in treatment of these patients.
References
- Horny HP et al. Systemic Mastocytosis. World Health Organization Classification of Digestive System Tumours (5th edition), p. 423-425, 2019
- Johncilla M et al: Are enterocolic mucosal mast cell aggregates clinically relevant in patients without suspected or established systemic mastocytosis? Am J Surg Pathol. 42(10):1390-5, 2018
- Doyle LA et al: A clinicopathologic study of 24 cases of systemic mastocytosis involving the gastrointestinal tract and assessment of mucosal mast cell density in irritable bowel syndrome and asymptomatic patients. Am J Surg Pathol. 38(6):832-43, 2014
- Cardet JC et al: Immunology and clinical manifestations of non-clonal mast cell activation syndrome. Curr Allergy Asthma Rep. 13(1):10-8, 2013
- Chiu A et al: Mastocytosis and related disorders. Semin Diagn Pathol. 29(1):19-30, 2012
- Ozdemir D et al: Systemic mastocytosis. Am J Med Sci. 342(5):409-15, 2011
- Sokol H et al: Gastrointestinal involvement and manifestations in systemic mastocytosis. Inflamm Bowel Dis. 16(7):1247-53, 2010
- Hahn HP et al: Immunoreactivity for CD25 in gastrointestinal mucosal mast cells is specific for systemic mastocytosis. Am J Surg Pathol. 31(11):1669-76, 2007
- Jakate S et al: Mastocytic enterocolitis: increased mucosal mast cells in chronic intractable diarrhea. Arch Pathol Lab Med. 130(3):362-7, 2006
- Siegert SI et al: Are gastrointestinal mucosal mast cells increased in patients with systemic mastocytosis? Am J Clin Pathol. 122(4):560-5, 2004
- Jensen RT: Gastrointestinal abnormalities and involvement in systemic mastocytosis. Hematol Oncol Clin North Am. 14(3):579-623, 2000