July 2020 Case
Authors
Chau Bui, MD (Resident), Fabiola Medeiros, MD (Faculty)
Gynecologic Pathology
Clinical History
This is a 55-year-old female with no significant PMH who presented with postmenopausal bleeding and bilateral sharp shooting pain in the pelvis. She underwent an endometrial biopsy, which demonstrated a müllerian mesenchymal neoplasm that could not be further classified based on histologic findings and immunostains. An NGS panel for sarcoma gene fusions was negative for gene rearrangements. Subsequent imaging revealed an enhancing mass centrally within the uterus extending into the endocervix. The patient underwent a total laparoscopic hysterectomy and bilateral salpingo-oophorectomy. On gross exam 5.0 x 3.0 x 2.5 cm tumor was found in the left side of the uterine corpus and did not involve the cervix.
Gross Features


Figure 1: A well-circumscribed polypoid, tan-yellow, soft tumor with no necrosis
Histopathologic Features
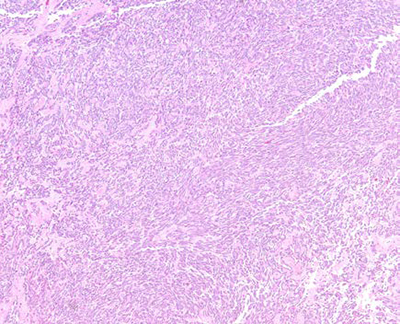
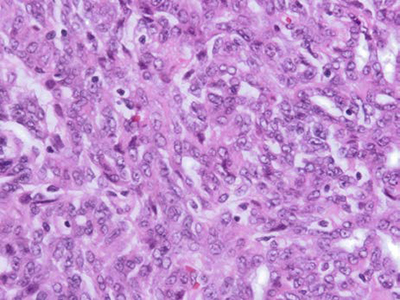
Figure 2. (H&E, 40x and 200x magnifications): Solid sheets of spindle cells with round to spindle nuclei, open chromatin and small nucleoli
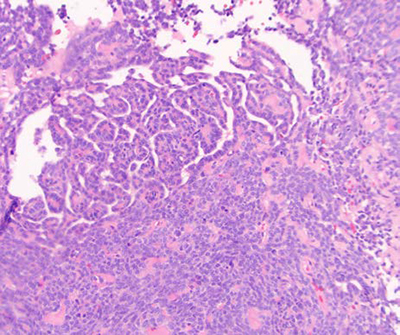
Figure 3. (H&E, 40x & 200x magnifications): Retiform architecture of epithelioid cells with hyaline material resembling a sex cord-like structure.
Immunohistochemistry

WT1
Calretinin

FOXL2
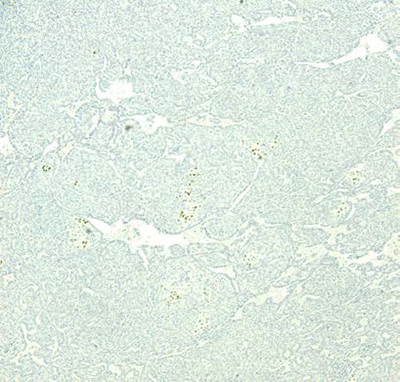
SF1
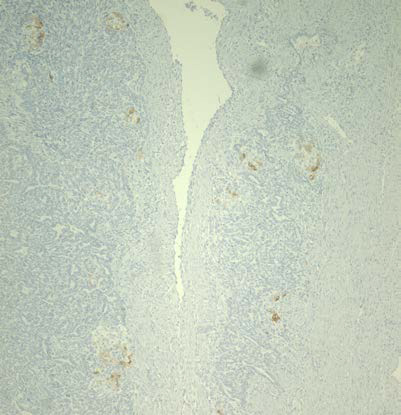
Inhibin

Melan-A
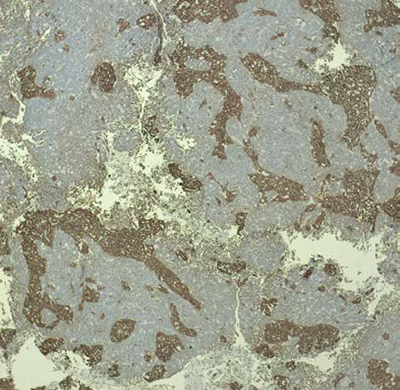
Figure 4: Immunohistochemical stains, sex cord markers
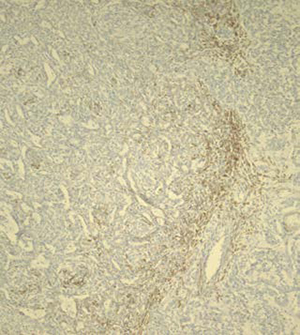
AE 1 & 3
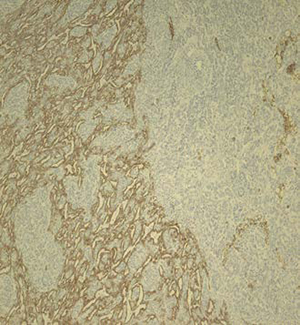
Desmin
CD10
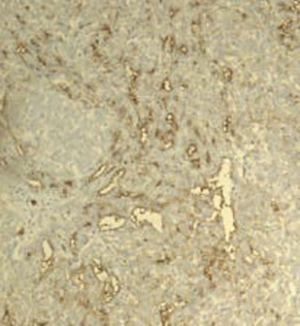
Figure 5. Additional immunohistochemical stains
Diagnosis
Uterine tumor resembling ovarian sex cord tumor (UTROSCT)
Discussion
UTROSCT is a rare uterine mesenchymal neoplasm that tends to occur in middle-aged women.
The tumor consists of sex cord-like and mesenchymal differentiation with various possible components, including Sertoli-like tubules, nested granulosa-like architecture, retiform growth, lipidized cells, Leydig-like cells, stromal cells with infiltrative growth, and solid sheets of smooth muscle-like cells. Occasional vascular invasion and necrosis can be seen. Mitotic activity is low, and cytological atypia is minimal.
UTROSCT expresses a variable immunoprofile with possible positive or negative staining for any of the commonly used sex cord markers, including inhibin, calretinin, SF1, WT1, and FOXL2. Co-expression of epithelial and muscle markers is common. UTROSCT is also typically positive for CD10 and less commonly positive for ER and PR. The differential diagnosis includes endometrial stromal tumor with sex cord-like differentiation, endometrial carcinoma with sex cord-like differentiation, adenosarcoma with extensive sex cord-like differentiation, and mesonephric adenocarcinoma. These entities can be distinguished based on a combination of histopathologic features, immunophenotyping, and molecular analysis.
Fusion genes found in UTROSCT include ESR1-NCOA3 (41%), GREB1-NCOA1 (18%), ESR1-NCOA2 (14%), and GREB1-NCOA2 (5%). Some adenosarcomas with extensive sex cord-like differentiation may also have a NCOA 2/3 gene fusion, which can render distinguishing between this entity and UTROSCT quite challenging. UTROSCT lacks FOXL2 and DICER1 mutations, which are found in granulosa cell tumors and Sertoli Leydig cell tumors of the ovary, respectively. UTROSCT also lacks JAZF1 and PHF1 rearrangements, which is helpful in differentiating UTROSCT from low grade endometrial stromal sarcoma.
UTROSCT has indolent behavior in most cases. Uncommonly, these tumors may behave aggressively and infiltrate the myometrium or through the serosa. Distant metastasis is rare but has been reported.
References
- Dickson BC, Childs TJ, Colgan TJ, Sung YS, Swanson D, Zhang L, Antonescu CR. Uterine Tumor Resembling Ovarian Sex Cord Tumor: A Distinct Entity Characterized by Recurrent NCOA2/3 Gene Fusions. Am J Surg Pathol. 2019 Feb;43(2):178-186. doi: 10.1097/PAS.0000000000001153hol. 2005 Feb;29(2):157-66.
- Goebel EA, Hernandez Bonilla S, Dong F, Dickson BC, Hoang LN, Hardisson D, Lacambra MD, Lu FI, Fletcher CDM, Crum CP, Antonescu CR, Nucci MR, Kolin DL. Uterine Tumor Resembling Ovarian Sex Cord Tumor (UTROSCT): A Morphologic and Molecular Study of 26 Cases Confirms Recurrent NCOA1-3 Rearrangement. Am J Surg Pathol. 2020 Jan;44(1):30-42.
- Jia M, Sun PL, Gao H3 Uterine lesions with sex cord-like architectures: a systematic review. Diagn Pathol. 2019 Nov 18;14(1):129.
- Kommoss F1, Schmidt D.Immunohistochemical sex cord markers. Description and use in the differential diagnosis of ovarian tumors
- Momeni-Boroujeni A, Chiang S. Uterine mesenchymal tumours: recent advances. Histopathology. 2020 Jan;76(1):64-75. Parra-Herran C, Howitt BE. Uterine Mesenchymal Tumors: Update on Classification, Staging, and Molecular Features. Surg Pathol Clin. 2019 Jun;12(2):363-396. doi: 10.1016/j.path.2019.01.004.